
 العربية
العربية Español
Español 中文
中文 Deutsch
Deutsch Français
Français Português
Português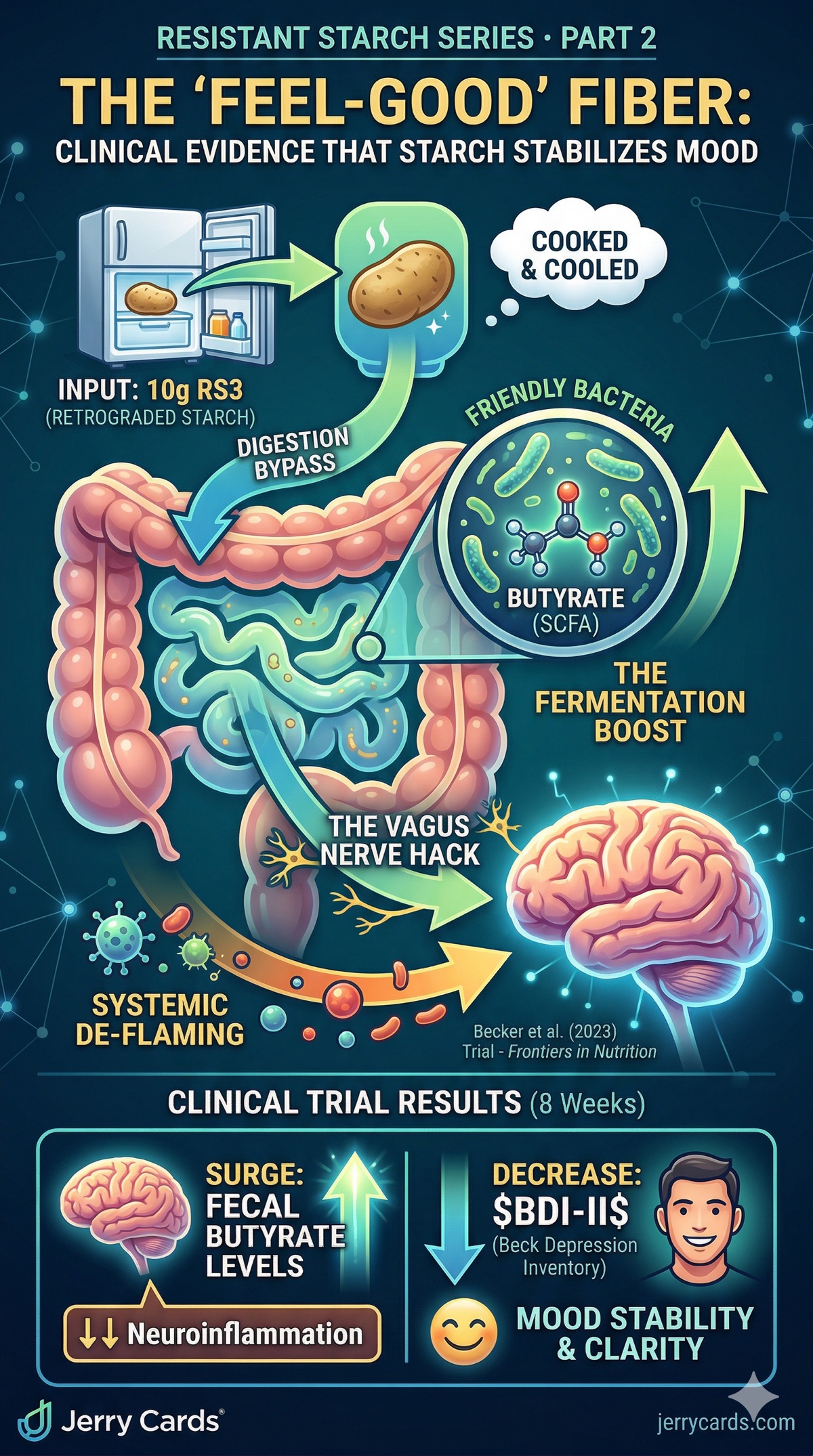
This is Part 2 of our Resistant Starch series. Part 1 covered the animal model evidence showing how RS reshapes the gut microbiome to improve cognition and mood via the gut-brain axis. Now we move to the question everyone asks: does this work in humans?
1. The RESISTA-PD Clinical Trial
The most compelling human evidence for resistant starch’s effects on mood comes from the RESISTA-PD trial (Becker et al.), an interventional, monocentric clinical trial funded by the Michael J. Fox Foundation for Parkinson’s Research.
1.1 Study Design
| Study Type | Interventional, monocentric, open-label clinical trial |
| Participants | 87 subjects in 3 arms: 32 PD patients + RS, 30 healthy controls + RS, 25 PD patients + dietary instructions only |
| Intervention | 5g resistant starch (RS3) twice daily = 10g/day total, for 8 weeks |
| Primary Endpoints | Fecal short-chain fatty acids (SCFAs), fecal calprotectin, gut microbiota composition |
| Secondary Endpoints | Beck Depression Inventory (BDI), non-motor symptom burden, gastrointestinal symptoms |
| Funding | Michael J. Fox Foundation for Parkinson’s Research |
1.2 Key Results
After 8 weeks of resistant starch supplementation:
| Outcome | Change | Significance |
| Depression Scores (BDI) | Significant improvement | p = 0.001 |
| Fecal Butyrate | Significant increase | p < 0.05 |
| Fecal Calprotectin (inflammation) | Significant decrease | p < 0.05 |
| Non-Motor Symptom Burden | Reduced | Clinically meaningful |
| Safety & Tolerability | Well-tolerated, no serious adverse events | — |
The BDI result is remarkable: p = 0.001 is a very high level of statistical significance for a dietary intervention. Most pharmaceutical antidepressant trials consider p < 0.05 as the threshold for significance.
2. The Biochemical Mechanism: Why Does a Starch Improve Depression?
The most important question for any scientist is not what happened, but why. The RESISTA-PD data, combined with recent mechanistic studies (2024–2025), reveals a clear multi-pathway causal chain from gut to brain.
2.1 Pathway 1: The Butyrate Anti-Inflammatory Cascade
The baseline problem: Patients with Major Depressive Disorder (MDD) have 40–60% less butyrate in their gut than healthy controls (Frontiers in Pharmacology, 2024). This butyrate depletion has been directly associated with the manifestation of depressive symptoms.
What RS does: Resistant starch is the single most effective dietary substrate for butyrate production. When fermented by gut bacteria (primarily Faecalibacterium prausnitzii, Roseburia, and Eubacterium rectale), RS produces more butyrate per gram than any other prebiotic fiber.
Butyrate then acts through multiple anti-inflammatory pathways:
- HDAC Inhibition: Butyrate is a potent histone deacetylase (HDAC) inhibitor — an epigenetic mechanism that downregulates pro-inflammatory gene expression. This is the same mechanism of action used by certain cancer drugs.
- NF-κB Suppression: Butyrate suppresses the NF-κB inflammatory signaling pathway, reducing the production of pro-inflammatory cytokines (IL-6, TNF-α, IL-1β) both in the gut and systemically.
- Blood-Brain Barrier Repair: Butyrate upregulates tight junction proteins (ZO-1, Occludin, Claudin-5) in the BBB endothelium, preventing inflammatory molecules from crossing into the brain.
2.2 Pathway 2: The Vagus Nerve Highway
The vagus nerve is the main physical conduit connecting the gut to the brain. It is composed primarily of afferent (gut-to-brain) fibers — approximately 80% of vagal fibers carry information upward from the gut to the brainstem.
- Butyrate activates vagal afferent neurons directly, triggering signaling cascades that reach the nucleus tractus solitarius (NTS) in the brainstem
- From the NTS, signals propagate to the hypothalamus (stress response), amygdala (emotional processing), and prefrontal cortex (executive function)
- The net effect: a "calm down" signal that reduces the hypothalamic-pituitary-adrenal (HPA) axis hyperactivity characteristic of depression
2.3 Pathway 3: Tryptophan Protection (The Serotonin Shield)
This pathway is perhaps the most elegant, and the most clinically relevant:
The problem: Tryptophan is the essential amino acid precursor to serotonin (the "feel-good" neurotransmitter). Under normal conditions, tryptophan is converted to serotonin via the TPH1/TPH2 enzyme pathway.
The inflammatory hijack: When systemic inflammation is high (elevated IL-6, TNF-α), the enzyme indoleamine 2,3-dioxygenase (IDO) is activated. IDO diverts tryptophan away from serotonin and into the kynurenine pathway, producing neurotoxic metabolites (quinolinic acid, 3-hydroxykynurenine) instead of serotonin.
What butyrate does: By reducing systemic inflammation, butyrate suppresses IDO activation, keeping tryptophan available for serotonin synthesis. Additionally, butyrate-producing bacteria like Faecalibacterium directly enhance TPH1 expression in gut enterochromaffin cells, boosting serotonin production at the source.
This is why the "chemical imbalance" theory of depression is being replaced by the "neuroinflammation" model. The imbalance isn’t random — it’s caused by inflammation diverting your tryptophan into the wrong pathway. Resistant starch addresses the root cause, not just the symptom.
3. The Complete Signaling Cascade
Resistant Starch (RS3)
↓
Colonic Fermentation by Faecalibacterium, Roseburia, Eubacterium
↓
↑ Butyrate + ↑ Propionate + ↑ Acetate (SCFAs)
↓ ↓ ↓
Path A: HDAC inhibition → ↓ NF-κB → ↓ IL-6, TNF-α → ↓ Systemic inflammation
Path B: Vagal afferent activation → NTS → ↓ HPA axis hyperactivity → ↓ Cortisol
Path C: ↓ IDO activation → ↑ Tryptophan → Serotonin (not kynurenine) → ↑ Mood
Path D: ↑ BBB tight junctions (ZO-1, Occludin) → ↓ Neuroinflammation in hippocampus
Path E: ↑ BDNF expression → Neuroplasticity → ↑ Cognitive resilience
↓
Outcome: Improved Depression Scores, Emotional Stability, Cognitive Clarity
4. Practical Translation: The Dose
The RESISTA-PD trial used 10g/day of RS3. What does that look like in real food?
| 1 medium potato, cooked then cooled 12–24 hours | ~8–12g RS3 |
| 1 cup cooked then cooled rice | ~3–5g RS3 |
| 1 cup cooked then cooled lentils | ~4–6g RS (mix of RS1+RS3) |
| 1 green (unripe) banana | ~5–8g RS2 |
| Bob’s Red Mill Potato Starch (supplement) | ~8g RS2 per tablespoon |
The key insight: You don’t need a supplement. One cooled potato or a combination of cooled rice + lentils provides the clinical dose. The cooling step is critical — it’s the process that converts digestible starch into RS3 (we’ll explain the physics of this in Part 3).
5. Supporting Evidence: The Broader Literature
The RESISTA-PD trial doesn’t exist in isolation. Several lines of converging evidence support the RS → butyrate → mood connection:
- Yang et al. (2023), Frontiers in Nutrition: A systematic review of prebiotics for depression found that butyrate-producing interventions (including RS) consistently reduced inflammatory markers and improved mood scores across multiple trials.
- Frontiers in Pharmacology (2025): A comprehensive review of "psychobiotics" identified resistant starch as one of the most promising dietary interventions for the gut-brain axis, with butyrate production as the primary mechanism.
- Butylated Starch Studies (2021–2024): Multiple rodent studies using chemically butylated starch (which delivers butyrate directly) showed significant reductions in depression-like and anxiety-like behaviors, confirming that butyrate itself — not just the fiber — is the active agent.
- The RICE Trial (NCT07152483): Currently recruiting — a dedicated clinical trial testing resistant starch intervention for cognitive enhancement in humans at high genetic risk for cognitive decline. Results expected 2026.
6. Limitations and Honest Caveats
No responsible analysis is complete without acknowledging limitations:
- Open-label design: The RESISTA-PD trial was not blinded, which introduces potential placebo effects. A double-blind RCT would provide stronger evidence.
- Disease-specific population: Participants had Parkinson’s disease, which has known gut-brain pathology. Results may not fully generalize to healthy populations.
- Sample size: 87 subjects is adequate for a pilot study but small by pharmaceutical standards.
- Direct causation vs. correlation: While the butyrate increase and BDI improvement occurred simultaneously, the trial design cannot definitively prove causation without a blinded control.
That said, the p = 0.001 significance level, combined with the mechanistic consistency across animal models and the broader literature, makes this a compelling signal that warrants larger trials.
7. What’s Next in This Series
- Part 3: The Kitchen Physics — Why cooling your food changes its molecular structure (RS2 vs RS3 vs RS4), and the exact temperature and time parameters for maximizing resistant starch content
- Part 4: The Brain Sharpness Menu — A practical 7-day meal plan with RS-optimized recipes
Sources: